Normalising gait data is so common that we may sometimes forget about why we are doing it. It’s getting on for 17 years since At Hof published his paper on non-dimensional normalisation (Hof, 1996). Slowly this approach is being becoming part of mainstream practice. What interests me, however, is how little testing to check that it actually works.
Normalisation is a technique to try and reduce the variability in data that comes when individuals of different sizes are being compared. A raw measure of joint moment in Newton-metres, for example, is likely to be greater in a heavier person simply because they are heavier. Measurements of joint moments across a range of people are likely to be vary considerably simply because those people are of different weights. By dividing all the measurements by bodymass and reporting measurements in N-m/kg we hope to reduce the variability. This should make it much easier to spot a subject who has abnormal moments because of the way they walk rather than how heavy they are.
At introduced a hypothesis that a particular way of normalising data to give non-dimensional values would reduce the variability in data. This is an extremely sensible approach but it is essentially a hypothesis. Given this it is interesting that there has been so little work to test the hypothesis. Ben Stansfield (2003) and colleagues in Edinburgh tested how non-dimensional normalisation affected a correlations between a range of temporal and spatial parameters with impressive results but didn’t actually address the even more basic question of how whether the normalisation reduces the variability with body size (which is what it is designed for as described above).
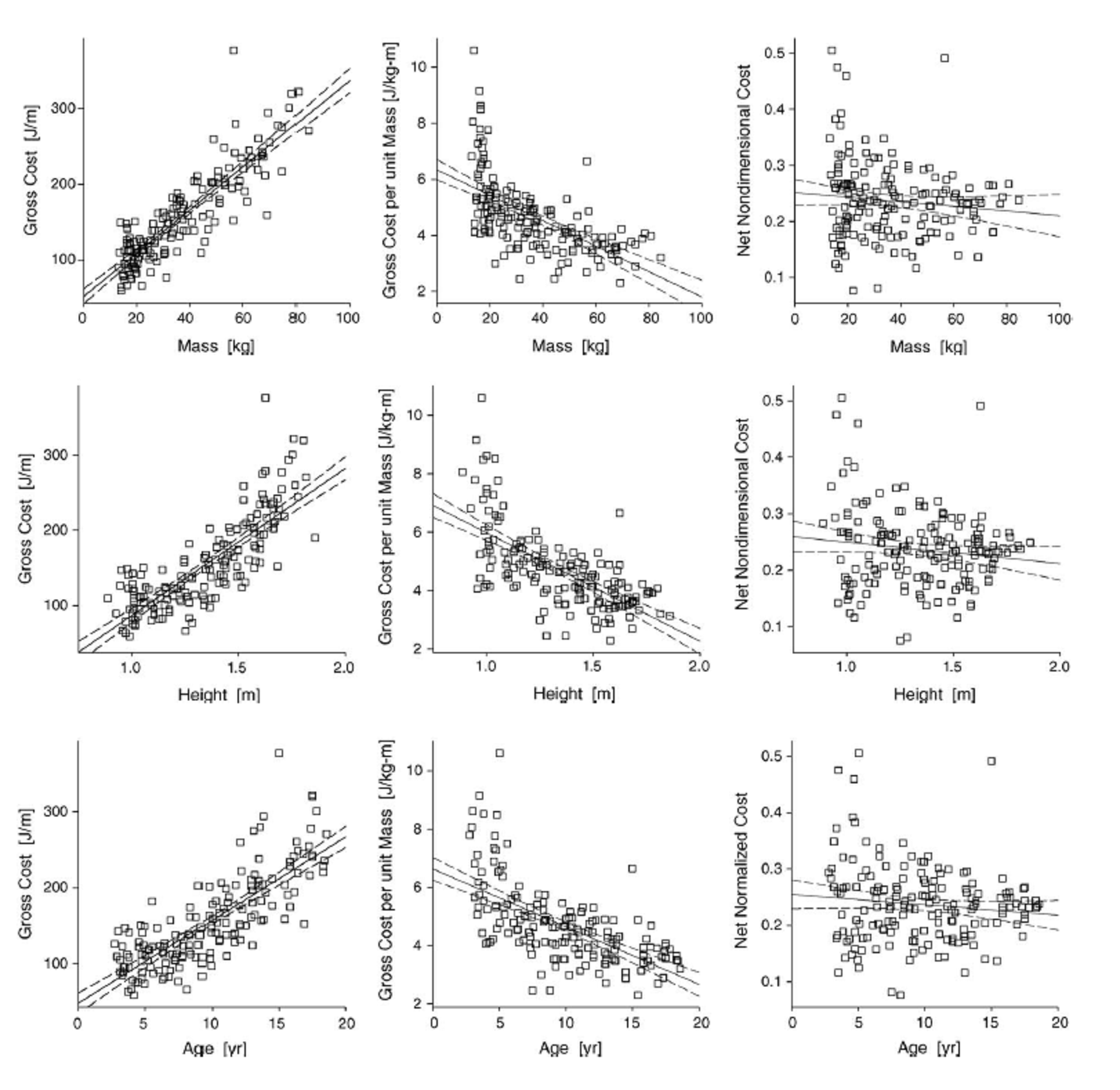
Adapted from Schwartz et al., 2006
Mike Schwartz and I (Schwartz et al., 2006) adopted the approach for normalising oxygen cost and rate/consumption. The traditional approach was simply to divide Oxygen cost by mass and when we tested this we found that the data was over-normalised. Raw measurements (mmO2/m) increase with increasing weight. Measures normalised by bodymass (mmO2/kg-m) actually decrease with increasing mass (see Figure below). Deriving a non-dimensional equivalent results in data that show no systematic variation with mass, height or age. When we did this paper I think we assumed that other people might investigate other normalisation schemes in a similar manner but, to my knowledge there have been no such studies.
Two obvious candidates for such studies are joint moments and powers. Dividing either by mass alone (as is almost universal practice in clinical gait analysis) only partially normalises the data. Hof recommends that moment should be normalised by leg length as well as mass (and this is common practice in some strands of research particularly studies of the knee adduction moment). It really is quite amazing that over three decades after David Winter popularised the use of joint moments in clinical gait analysis (Winter & Robertson, 1978) no-one yet has performed a definitive study to identify the optimum normalisation scheme for the data.
Hof, A. (1996). Scaling gait data to body size. Gait and Posture, 4, 222-223.
Schwartz, M. H., Koop, S. E., Bourke, J. L., & Baker, R. (2006). A nondimensional normalization scheme for oxygen utilization data. Gait Posture, 24(1), 14-22.
Stansfield, B. W., Hillman, S. J., Hazlewood, M. E., Lawson, A. M., Mann, A. M., Loudon, I. R., & Robb, J. E. (2003). Normalisation of gait data in children. Gait Posture, 17(1), 81-87.
Winter, D., & Robertson, D. (1978). Joint torque and energy patterns in normal gait. Biological Cybernetics, 29, 137-142.


