There was some discussion at the CMAS meeting in Glasgow last week about what causes the characteristic bumps in the vertical component of the ground reaction. Before you read on it might be worth just stopping to think this through for yourself. Working from the premise that Newton declared that if there is a net force acting on an object then it must be accelerating – which acceleration does the first bump represent and which bump does the second represent?
Several of us admitted to believing that the prevailing wisdom (“what the textbooks say”) is that the first bump represents a deceleration of the centre of mass as it’s downwards movement is arrested and that the second bump is the upwards acceleration as we push off. This is not the correct explanation as Barry Meadows made clear in his presentation.
I’ve plotted some idealised data below to illustrate what is actually happening. The ground reaction under the left limb is represented in red and that under the right limb in right. One thing we should do more often is to plot the sum of these which of course is the total force acting on the body (Chris Kirtley does do this in his book, 2006). The first interesting thing to note is that the peak total ground reaction actually occurs just before the middle of double support where two relatively modest forces from the different limbs superimpose.
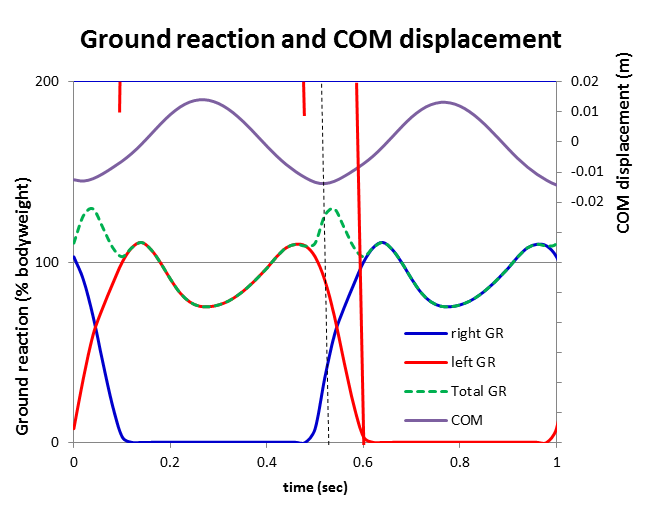
I’ve also plotted the trajectory of the centre of mass (calculated from a double integration of the total ground reaction). It is at its highest in middle single support and lowest in early double support. The dotted black line shows its minimum value. Before this point the COM is travelling downwards and being decelerated and afterwards it is travelling upwards and being accelerated. Thus the first bump of the ground reaction is acting to accelerate the body upwards and the second bump is acting to decelerate as it falls from its peak height during middle single support. This is the opposite to “what the text books say”.
Or are we being unfair to the text books? I’ve gone back to see.
Whittle (2012) and Kaufman and Davis (writing in Rose and Gamble, 2006) get the explanation spot on.
Gage(2009, p54), on the other hand, states that the “body has been accelerating by gravity as it fell from its zenith at mid-stance to its nadir at loading response. As a result the total force on the limb as it impacts the floor is about 120% of body weight“. This is a bit vague but essentially wrong. The body has actually been decelerating for half of its fall from zenith to nadir such that the vertical component of its speed is virtually zero at foot contact. The first peak of the ground reaction occurs well after the limb impacts the floor and is a result of the centre of mass being accelerated upwards.
Perry (2010, p459) writes that “the first peak (F1) … is increased above bodyweight by the acceleration of the rapid drop of the body mass”. This is also wrong- the deceleration of the body mass is almost complete by initial contact and has occurred as a consequence of the GR under the trailing limb. The description of the second peak is even more confused – “the second peak (F3) … is modified by the push of the ankle plantar flexor muscles against the floor in addition to the downward acceleration of the COG as the bodyweight falls forwards over the forefoot rocker“.
So there we have it on a random sample of four books that happen to be on my shelf this afternoon two have the explanation correct and two have it essentially wrong.
There is some additional confusion because the fore-aft component of the ground reaction actually has the opposite effect. In the first half of stance the GR is acting to decelerate the body in a horizontal direction (at the same time as accelerating it in an upwards direction). In the second half of stance the opposite is occurring as the GR is accelerating the body forwards (at the same time as it is decelerating it as it falls vertically).
.
Kirtley, C. (2006). Clinical gait analysis (1st ed.). Edinburgh: Elsevier
Levine, D., Richards, J., & Whittle, M. W. (2012). Whittle’s Gait Analysis (5th ed.): Churchill Livingstone.
Rose, J., & Gamble, J. (Eds.). (2006). Human Walking (3rd ed.). Philadelphia: Lippincott Williams and Wilkins.
Perry, J., & Burnfield, J. M. (2010). Gait analysis: normal and pathological function (2nd ed.). Pomona, California: Slack.
Gage, J. R., Schwartz, M. H., Koop, S. E., & Novacheck, T. F. (2009). The identification and treatment of gait problems in cerebral palsy (1st ed.). London: Mac Keith Press.