It’s fifteen years since the publication of the first paper on the GMFCS (Palisano et al., 1997). Since then it has become ubiquitous in the field of cerebral palsy. More and more measures are being found that correlate with it. It just seems like magic. But the more things we discover that show this correlation the more I wonder whether this really is magic. Have we missed something? Are we asking the right questions?
Cerebral palsy is an extremely heterogeneous condition affecting some kids extremely severely and others very mildly. In terms of gross motor function the range is from a child with hemiplegia and a mild foot drop right through to those with severe total body involvement who are essentially immobile. GMFCS allows us to group children (and now adolescents, Palisano et al., 2008) in terms of that function. In other words, GMFCS is essentially a classification of the severity of CP as indicated by gross motor function.
When we think about it most of the other indices, scores and scales we look at can be considered to be measures of the severity of CP as indicated by other aspects of the condition. When we get a correlation between GMFCS and another measure we are thus really saying there is a correlation of the severity of CP indicated on the basis of Gross Motor Function and severity of CP as indicated by hip dysplasia (Robin et al., 2008, see Figure below) , or gait quality (Baker et al., 2009) or physical activity (Bjornson et al., 2007). We shouldn’t really be surprised that there is a correlation – in fact the thing that should really surprise us is if there isn’t.
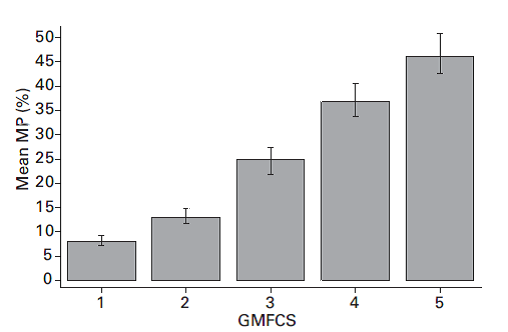
Correlation of hip dysplasia (migration percentage) with GMFCS (Robin et al., 2008)
A more nuanced approach to research in CP might be to anticipate the underlying correlation between indicators of severity of CP and accept it as unremarkable. Measures that don’t correlate are actually more remarkable and further investigation of these, when they are identified, might be more productive than investigation of those that do. Detailed consideration of individual children that buck the trends may also give important clinical insights.
.
Baker, R., McGinley, J. L., Schwartz, M. H., Beynon, S., Rozumalski, A., Graham, H. K., & Tirosh, O. (2009). The gait profile score and movement analysis profile. Gait Posture, 30(3), 265-269.
Bjornson, K. F., Belza, B., Kartin, D., Logsdon, R., & McLaughlin, J. F. (2007). Ambulatory physical activity performance in youth with cerebral palsy and youth who are developing typically. Phys Ther, 87(3), 248-257.
Palisano, R., Rosenbaum, P., Walter, S., Russell, D., Wood, E., & Galuppi, B. (1997). Development and reliability of a system to classify gross motor function in children with cerebral palsy. Dev Med Child Neurol, 39(4), 214-223.
Palisano, R. J., Rosenbaum, P., Bartlett, D., & Livingston, M. H. (2008). Content validity of the expanded and revised Gross Motor Function Classification System. Dev Med Child Neurol, 50(10), 744-750.
