I’m teaching about gait to the undergraduate physios next week. Its the first lecture I’ve given at this level trying to emphasise the approach I’ve developed in the Why we walk the way we do videos. The colleague who’s delivering the previous lecture – which included a first introduction to gait graphs – wanted to use the same format as I use which started a conversation about what aspects of walking we’d like those graphs to emphasize.
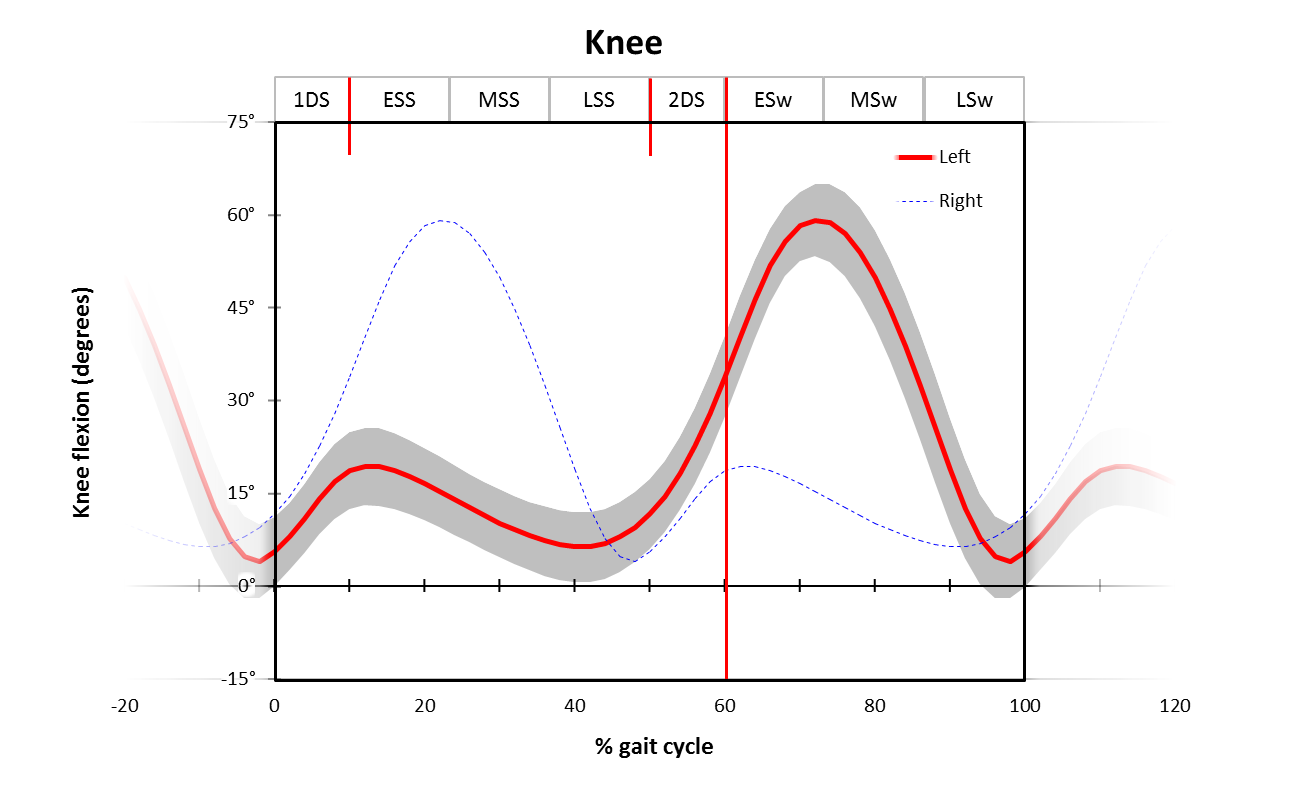
I’m pretty keen on fixed aspect ratios and scaling so that you can forget about those issues when you are actually looking at data – so we’ve fixed that. We wanted also wanted to reinforce the terminology for different phases that I’ve described in a previous post – so we’ve put those abbreviated names across the top.
I also like to represent the continuity of the gait cycle – it amazes me how many people I come across who don’t seem to realise that point on the far left of the graph is the same as the point on the far right hand side (give or take a little stride to stride variability). It’s also not uncommon to spot data in the literature where values of gait variables at 0% and 100% are different but not commented upon. Various people in the past have tried plotting more than a single stride to try and emphasize continuity. I know Jurg Baumann was an advocate of this but can’t find easily get my hands on a sample. At Hof also used it – his 2002 paper on the speed dependence of EMG profiles is an example – but it has never really caught on. In this format I’ve tried to capture the point by allowing the gait curves to fade away to nothing outside the graph. It’s a bit messy if you’ve got a whole array of graphs but I kind of like it in the context of an introduction at this level.
I’m also very keen on getting students to appreciate what the right leg is doing plotted on the same time scale as the left leg. I know this insenses people who are paranoid about the importance of symmetry in gait but it’s a hell of a lot easier to explain the biomechanics if you look at the data this way. It’s unconventional of course so I’ve chosen to represent this as a much fainter line.
There was another question mark over the hip angle. As gait analysts most of us assume that this should be measured relative to a pelvic axis represented by the line from PSIS to ASIS and thus biasing the hip graph towards flexion. In assessing gait by observation, however, physios almost always consider the angle with the vertical which might be more relevant for daily practice. In the end we decided to stick with the gait analysis approach and just make sure we explain this very clearly.
Anyone got any additional features they like to add?
.
Hof, A. L., Elzinga, H., Grimmius, W., & Halbertsma, J. P. (2002). Speed dependence of averaged EMG profiles in walking. Gait Posture, 16(1), 78-86.