If readers don’t recognise this diagram then they should. It comes from the World Health Organisation’s International Classification of Functioning , Disability and Health (ICF). It proposes a model within which to consider how any health condition affects a person’s life. It’s becoming an important tool to plan research on the assumption that interventions to improve people’s walking ability should be assessed over a range of levels.
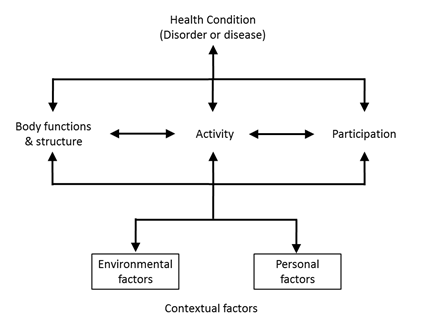
It assumes that the affect that a health condition has on a person’s life depends on a balance between attributes of the health condition itself and a range of contextual factors which can relate to the environment in which the person lives of be personal characteristics. Thus the life of a person who cannot walk (health condition) will be affected by environmental factors such as whether they have a wheelchair and whether the places they want to visit are wheelchair accessible and personal factors such as motivation or coping abilities.
Three levels are used to describe the person relate to the body or a body part (body structure and functions), the whole person (activity) and the whole person within a societal context (participation). Factors affecting body structure and function interact with those affecting activity (this is a two way interaction – horizontal arrows). Those affecting activity also interact with those activity interact with participation. Note that there is no direct interaction between body structure and function and participation – I’ll pick this up in a later post).
Another aspect of the classification is a distinction between capacity, what a person is able to do within a standardised environment, and performance, what they actually do in their current environment. Thus we have come across children with disability who have the capacity to walk with crutches, but perform as wheelchair users because some schools consider this to be safer.
If we just look at this diagram it’s not at all clear where walking fits in. Most people don’t look any further than the diagram which means there is some ambiguity in the literature considering walking within the context of the ICF. The ICF is not limited to the diagram however and contains an entire classification system (as the name suggests!). Perhaps the easiest way to get your head around the classification itself is to use the illustrated version.
")
Images from the illustrated ICF (click on picture to take you there)
In this the gait pattern is listed as item b770 in the Neuromusculoskeletal and Movement Related Functions chapter. It thus becomes very clear that walking as measured by a gait analysis service is an example of a body function (and more specifically that the measures are of capacity – you don’t get a much more standardized environment than a gait analysis laboratory).
Walking as it occurs as part of everyday life is defined as an activity within the Mobility chapter of the ICF. It is further divided into walking over different distances (d4500 & d4501), on different surfaces (d4502) and around obstacles (d4503). For most people walking will be the main method of moving around the home (d4600), in other buildings (d4601) and for short distances outside the home (d4602). By definition this activity cannot be measured within the gait laboratory but questionnaires or data logging devices can be used to obtain the information. The Functional Mobility Scale (Graham, 2004) , for example, assesses dependence on walking aids over three distances, 5m, 50m and 500m which fits nicely onto categories d4600, d4601 and d4602 (although I don’t think any of the team were conscious of this when the scale was being developed).
How a person’s participation in society will clearly be affected by their walking ability but is not covered by any specific codes within the ICF.
.
PS
The history of the development of the ICF (and its predecessor, the ICIDH) makes interesting reading. It is the result of an ongoing discussion as to whether health should be primarily viewed using a medical or social model (see the Beginner’s Guide or the article in the International Encyclopaedia of Rehabilitation). The two classifications also marked a transition from the WHO’s original focus on preventable deaths (which are still the primary health concern in many of the world’s poorest countries) to what represents health (which is much more comfortable for those of us in richer countries). This rarely gets written about but then again most people doing the writing are doing so from within the richer countries!
.
PPS in writing this post I spotted the first error in my book – the horizontal arrows are missing from the version of the ICF diagram (Figure 9.1). Do let me know if you find others.
.
Graham, H. K., Harvey, A., Rodda, J., Nattrass, G. R., & Pirpiris, M. (2004). The Functional Mobility Scale (FMS). J Pediatr Orthop, 24(5), 514-520.
