Quite out of the blue Jenny Kent from Headley Court asks if I know where the gait graphs we know today come from. She was particularly interested in where the idea of time normalising data to the gait cycle originated. I have to admit I just don’t know.
Braune and Fischer, working at the end of the 19th century, certainly plotted a number of gait variables against time, most for swing but a few for more than a gait cycle. All the graphs I can see though plot these against time rather than a percentage of the gait cycle and the data for more than a gait cycle doesn’t appear to be plotted in relation to the gait events at all.
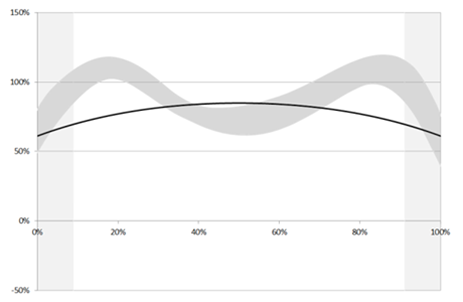
The first group that I can find that present variables on graphs with the time axis labelled as % gait cycle is Inman’s group working in Berkeley in the early 1950s.

Data scanned a long time ago from one of the outputs of the Berkeley group – not sure which.
Can anyone provide any earlier examples?
.
This made me think about other features of our standard gait graphs. Who first proposed plotting data from a patient against normative reference data depicted as a mean and range based on the standard deviation?
I remember that when the Vicon Clinical Manager software came out in 1992 that it assumed that all data was normalised to the gait cycle (the data was actually stored in a .gcd file on this assumption). The software only allowed three traces to be plotted on any graph so the common practice was to plot the mean of the reference data along as one right and one left side trace for each patient. I think the practice of plotting several (three!) traces from each side separately to assess measurement variability probably dated to this time as well. I don’t remember the standard deviations being plotted but this may just be my memory (the standard deviation values could certainly be stored in the .gcd file).
I also remember being impressed by teaching material from Newington and Gillette Hospitals (Gage, Davis and Ounpuu) which plotted the standard deviation ranges from quite an early stage. Looking up some of their early papers I find that Sylvia’s 1995 paper contains sample patient data plotted against the standard deviation ranges. (Unfortunately the quality of this figure in the .pdf file I have is too poor to be worth reproducing here).
Sylvia moved to Newington from Waterloo so I wondered how David Winter had plotted his data. Sure enough in the final chapter of The Biomechanics and Motor Control of Human Walking (1991) entitled “Assessment of pathological gait” are a series of graphs showing gait variables from a patient with a knee replacement plotted against the mean and standard deviation from a reference population. (This book was an adaptation of an earlier one form 1987 which I don’t have access to and I’d be interested to know if these graphs were included in that as well).
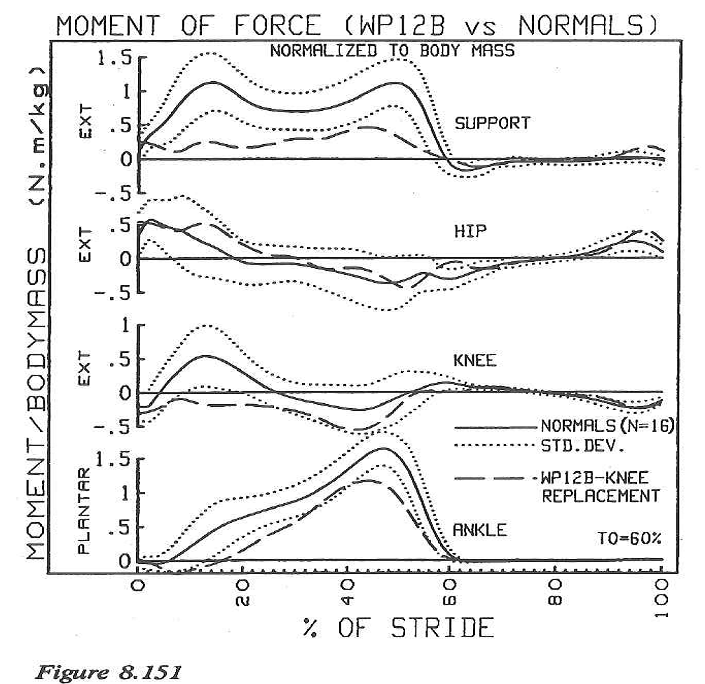
I’d like to suggest that this might be the earliest example of gait graph as we use them today – or has anyone got any earlier examples?
Of course tracing ideas back like this is a slightly ridiculous activity because such graphs often appear in publications only after having been used more generally for a considerable period. Just because they first appear in print from one team does not necessarily mean that they originated there!
.
Braune, W., & Fischer, O. (1987). The Human Gait (P. Maquet & R. Furlong, Trans.). Berlin ; New York: Springer-Verlag.
Klopsteg, P. E., & Wilson, P. D. (1954). Human Limbs and their Substitutes. New York: McGraw-Hill.
Ounpuu, O., Davis, R., & Deluca, P. (1996). Joint kinetics: Methods, interpretation and treatment decision-making in children with cerebral palsy and myelomeningocele. Gait and Posture, 4, 62-78.
Winter, D. (1991). The biomechanics and motor control of human gait: Normal, Elderly and Pathological (2nd ed.). Waterloo:: Waterloo Biomechanics.
")