While still reflecting on the way we use terminology so misleadingly within gait analysis it might be worth thinking a little about the concept of external work. It’s a concept that is even older than I am. Although previous workers (notably Fenn and Elftman) had used similar concepts it was Giovanni Cavagna who popularised it with his classic paper from 1963. (Cavagna et al. 1963). The article starts with the sentence, “The work performed in walking can be considered as being made of two components, the internal work and the external work”. My response to this is that you can consider it like that if you want but you are likely to confuse people if you do!
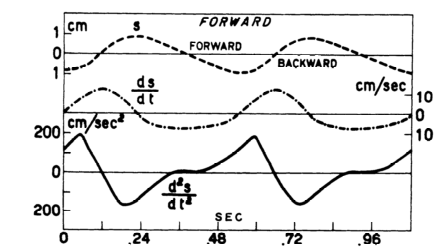
Graphs from Cavagna’s 1963 paper showing how horizontal components of speed and displacement are calculated from acceleration data. Note that his data was taken from an accelerometer worn on the body whereas it is more common these days for similar techniques to be used based on force plate measurements.
Let’s be clear that there is no external work in walking. All the work required for walking is generated internally by the muscles. The result of muscles (and ligaments) exerting forces on the skeleton is that the foot exerts a force against the floor and generates the ground reaction (following Newton’s third law) but the ground reaction itself doesn’t do any work. It can’t. In order for a force to do work the point of application needs to move and the ground doesn’t move (well, not very often).
Whether its name is correct of not, the concept is important because it allows an estimate of the energy cost of walking on the basis of force plate measurements alone (cuts out all that nasty kinematics). The theory behind the calculations is generally presented as straightforward but actually requires some quite subtle reasoning.
Although the ground reaction doesn’t do any work, it is a force applied externally to the body and will result in the centre of mass of the body being accelerated (Newton’s first law). If we measure the ground reaction we can thus calculate this acceleration and thus how the centre of mass is moving (its velocity and displacement).
Now if we wanted to move an equivalent mass through the same trajectory we could do so by applying an external force of the same magnitude and direction as the ground reaction directly to its centre of mass. If we did this then the point of application of this imaginary force would move and it would do work. Knowing the laws of physics it is reasonably easy to calculate what this work would be.
This can be taken as equivalent to the work that the muscles have to do to move the centre of mass, but it should be emphasized that the external force applied at the centre of mass is entirely imaginary, for the purposes of the calculation only. All the work is done internally by the muscles.
Of course this is one of those areas where people who understand the underlying concepts can cope with the fact that the name is wrong and get on with life … but I suspect that the terminology has the potential to be extremely misleading for those who don’t.
Additional note. It may also be worth being explicit that the muscles do other things as well as moving the centre of mass. They also move the segments with respect to the centre of mass and the work required to do this is not captured in the calculation outlined above. The calculation will thus always be an under estimate of the true mechanical cost of walking. It’s interesting that despite the extent to which these techniques have been used there have been very few studies of how much of an under-estimate, either for normal walking or for walking with pathology of different kinds.